Herpetic, or herpes, angina in a child has synonyms "enteroviral vesicular pharyngitis", "herpangina", "enteroviral vesicular stomatitis", which is due to the effect of a certain pathogen, as well as the nature of pathological rashes resembling herpes. However, the term "angina" in this case is due solely to the presence of pain in the throat, since the nature of the lesion and even its localization does not correspond to the signs of acute tonsillitis, both streptococcal and viral in nature.
 This infectious disease is widespread due to airborne transmission of the pathogen. A very typical method of infection is also the alimentary and contact route, when, if hygienic conditions are not observed, pathogens enter the body through the mouth, exerting a pathogenic effect on the mucous membrane of the throat. In children, this path is possible when using household items and toys that are contaminated with saliva or secretions from the nasopharynx.
This infectious disease is widespread due to airborne transmission of the pathogen. A very typical method of infection is also the alimentary and contact route, when, if hygienic conditions are not observed, pathogens enter the body through the mouth, exerting a pathogenic effect on the mucous membrane of the throat. In children, this path is possible when using household items and toys that are contaminated with saliva or secretions from the nasopharynx.
In this case, the infected patient becomes dangerous to others even before the first signs of angina appear, as well as during the first 7 days of the height of the disease. Further, its infectiousness decreases. The high contagiousness of the disease is a reason for a close study of its symptoms and the search for methods to combat it.
Disease periods
Like any infectious disease, herpes sore throat in children has different periods in its development, characterized by certain symptoms:
- incubation;
- premonitory;
- the peak period of clinical signs;
- recovery.
The incubation period usually lasts 7-14 days. This interval corresponds to the time from the moment of infection until the first signs of the disease appear.
After this time, a prodromal period begins, characterized by nonspecific signs characteristic of many other pathological processes. Most often, there are complaints of weakness, malaise, headache, decreased appetite, the development of subfebrile condition.
Sore throat, salivation, runny nose, dry cough are noted somewhat later in the prodromal period. Objective examination of the pharynx reveals slightly enlarged and hyperemic tonsils, redness of the mucous membrane of the hard and soft palate. In newborns, this condition can be manifested by irritability, refusal to eat. This symptomatology lasts, on average, 1-2 days.
The prodromal period is replaced by the height of the disease, when clinical symptoms are most clearly manifested. Herpetic sore throat in a child is manifested by the following mandatory signs:
- pain in the throat, aggravated by swallowing;
- the presence of characteristic rashes in the throat;
- enlargement and soreness of regional lymph nodes;
- an increase in body temperature up to 40 degrees.
Unlike the pain syndrome typical for tonsillitis, the nature of the pain in herpes sore throat in children is not compressive. Adults describe it as a stabbing sensation that intensifies not only when swallowing, but also when irritated by food or liquid.
During the height of the disease for this pathology, there are frequent signs indicating the involvement of the gastrointestinal tract in the process:
- nausea;
- abdominal pain;
- diarrhea;
- vomit.
The presence of these symptoms is due to the effect of a specific pathogen, an enterovirus. Occasionally, there may be rashes on the arms and legs that resemble a herpetic rash. They remain on the skin for 1-2 days, then regress without a trace.
Characteristics of lesions
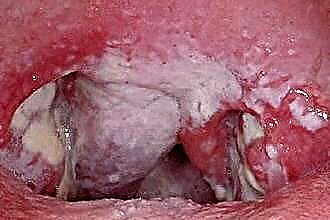
Herpes sore throat in children, or vesicular pharyngitis, is characterized by the presence of typical rashes on the throat mucosa. In this case, the most characteristic places of localization are not only the tonsils, but the posterior wall of the pharynx, arch, hard and soft palate, which distinguishes this pathology from various acute tonsillitis. An objective examination reveals a bilateral lesion.
By the nature of the rash, pathological foci are single reddish bubbles filled with translucent contents. They are 1–2 mm in diameter. The number of pathological foci usually does not exceed 10-12 and is proportional to the severity of the disease. These formations are very painful, which aggravates the patient's condition, interferes not only with food intake, but also with fluid intake.
A few hours after its appearance, the liquid in them brightens, they become like a herpetic rash, which is the reason for the name. After 2-3 days, the bubbles open, the liquid in them flows out. In their place, an erosive surface forms, which persists for several days. Shrinking, erosion is transformed into crusts, and then washed off with saliva.
In this way, the mucous membranes are cleared. The disease enters the next stage, recovery. At this stage, the general condition of the patient improves, the temperature indicators are normalized. Gradually, the mucous membranes of the pharynx, tonsils take their previous appearance. Herpetic sore throat in children lasts for 7-10 days. However, there are frequent cases of a longer course of the disease.
Features of the course in children under one year old
This disease is most typical for children aged 3 to 10 years. In children under one year old, as well as weakened patients, herpangina can be characterized by a more severe course and the presence of such additional signs:
- conjunctivitis;
- muscle pain;
- inflammatory processes in the kidneys;
- heartache.
In some weakened children, there may be a cyclical development of pathological foci, when new vesicles appear to replace the opened vesicles. Each time this development is accompanied by a new rise in temperature. However, in most cases, despite such a long course, the prognosis of the disease is favorable.
A recurrent course for herpangina is uncharacteristic.
Complications
The development of complications is more often due to the addition of a secondary bacterial infection. In this case, a change in the clinical picture is characteristic. Against the background of the outlined improvement in the general condition, a decrease in body temperature, there is an increase in pain in the throat, a new temperature jump.
Pharyngoscopy allows you to detect a change in the nature of the pathological focus. Serous translucent contents are transformed into yellowish-purulent foci. A general blood test, carried out during this period, reveals the presence of leukocytosis, a shift in the leukocyte formula to the left, as well as an increase in ESR up to 30 mm / h. Such a change in the clinical picture is an important factor requiring correction of treatment.
A much rarer complication of the disease is the development of meningitis. This complication is due to the spread of the process. In addition to hard membranes, brain tissue can also be involved in the process, which will lead to the development of encephalitis, and the inflammatory process can also affect the heart muscle, leading to the development of myocarditis.
Diagnostics
Diagnosis of the disease is usually straightforward. From herpetic stomatitis, which is also manifested by the presence of pathological foci on the mucous membranes and high hyperthermia, herpetic sore throat in a child differs in the localization of the lesion. Despite the similarity of pathological foci, the involvement of the mucous gums and tongue in the process is characteristic of stomatitis.In addition, for children aged three to four years, it is more typical to damage the pharynx, tonsils and palate, that is, the development of herpes sore throat. Stomatitis in children of this age is less common; it usually occurs up to three years of age.
From purulent sore throat, characterized by the development of single foci on the follicles, herpes sore throat also differs in localization.
Purulent lesion of the tonsils with follicular angina is determined only within the lymphoid tissue, without spreading to adjacent tissues.
In addition, with purulent angina, symptoms such as a runny nose, dry cough, characteristic of a viral lesion, are atypical.
In cases where the diagnosis is doubtful, laboratory tests are carried out to reliably identify the pathogen. The most relevant in this case is serological diagnostics, which allows detecting the presence of antibodies to these pathogens (ELISA, RNGA, RSK), as well as PCR diagnostics aimed at detecting the pathogen in the contents of the pathological focus.