The degree of violation of tracheobronchial conduction is determined by endoscopic examination, spirometry and radiation techniques - tomography, radiography.
The degree of violation of tracheobronchial conduction is determined by endoscopic examination, spirometry and radiation techniques - tomography, radiography.
The pathological changes in the tissues of the trachea are based on functional and organic defects of the respiratory tract.
The real cause of the occurrence of organic stenotic lesions of the ENT organs is unknown, while functional disorders account for only 1/5 of the total number of diagnosed tracheostenoses.
Etiology
The trachea is a hollow cartilaginous tube that sits between the larynx and the bronchial tree. It plays a key role in carrying air from the mouth and nasal cavity to the lungs. Inside the hollow organ, there are lymphoid tissues and special glands that protect the mucous membranes of the ENT organs from drying out. Narrowing of the inner diameter of the tube leads to the development of respiratory failure. Against the background of oxygen deficiency in the body, disturbances occur in the work of the cardiovascular, nervous and respiratory systems.
Why is there a narrowing of the trachea? There are several provoking factors that contribute to stenotic damage to the airway:
- congenital anomalies;
- chronic inflammation of the ENT organs;
- thermal and chemical burns of mucous membranes;
- cicatricial changes in tissues;
- tumors of the mediastinum;
- neoplasms on the thymus (thyroid) gland;
- complications after tracheostomy.
Mechanical trauma very often causes the development of cicatricial stenosis. Damage to the mucous membranes of the respiratory tract entails a violation of tissue trophism.
After the trachea is restored, scars form in it, which narrow the inner diameter of the airways and thereby interfere with normal breathing.
Chemical and thermal burns, frequent relapses of respiratory diseases, neoplasms in the throat and tracheostomy are the key causes of the development of tracheostenosis.
Symptomatic picture
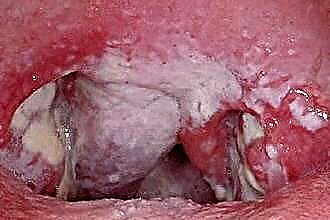
The manifestations of stenosis are determined by the degree of narrowing of the lumen in the airways, the etiology of the disease and associated complications. The most striking picture of tracheostenosis is observed when the inner diameter of the hollow organ is narrowed by more than 2/3. In any case, stenotic lesion of the ENT organs is accompanied by a disorder of respiratory function, inflammation in the mucous membranes of the trachea and hypoventilation of the lungs.
Typical manifestations of stenosis include:
- stridor (wheezing breathing);
- paroxysmal cough;
- cyanosis of the lips and limbs;
- "Marbling" of the skin;
- lowering blood pressure;
- dyspnea (shortness of breath);
- an increase in the amount of phlegm in the throat.
The narrowing of the lumen in the trachea leads to a violation of gas exchange due to a lack of oxygen in the tissues and the accumulation of carbon dioxide in them. To compensate for the O2 deficiency in the body, a person begins to breathe more often.
Physical activity only aggravates the patient's well-being and causes dizziness, nausea, muscle weakness, etc.
 With functional impairment of the airway patency, patients develop a cough-fainting syndrome. With a slight narrowing of the trachea, a spastic cough occurs, which intensifies over time.
With functional impairment of the airway patency, patients develop a cough-fainting syndrome. With a slight narrowing of the trachea, a spastic cough occurs, which intensifies over time.
At the peak of a coughing attack, nausea, dizziness, respiratory arrest, and even loss of consciousness appear. On average, the duration of fainting is 2 to 5 minutes.
In severe cases, bouts of violent coughing lead to collapse of the lung and death.
Varieties of tracheostenosis
Depending on the etiology of the development of the disease, tracheostenosis can be functional or organic. Organic stenoses are divided into primary, which are associated with morphological changes in the trachea, and secondary, i.e. arising from compression of the airways from the outside.
As a rule, the primary tracheal stenotic lesion is caused by the formation of scars in the cartilaginous and soft tissues. Cicatricial deformities often occur after operations, tracheostomy and foreign bodies entering the ENT organs.
Sometimes tracheostenosis appears due to nonspecific inflammation of the respiratory tract. Functional stenosis often develops against the background of spinal deformity, bite changes and flat feet.
Compression stenosis develops as a result of compression of the airways by mediastinal tumors, enlarged submandibular lymph nodes, hypertrophied thyroid gland, or bronchogenic cysts. Congenital tracheostenosis occurs due to the partial closure of the cartilaginous rings or hypoplasia of the membranous parts of the trachea.
Cicatricial tracheostenosis
Cicatricial tracheal stenosis is a deformation of the tracheal framework associated with the replacement of structural elements of the organ with scar tissue. Pathology most often develops due to compression of the walls of the cartilaginous organ with a tracheostomy cannula or endotracheal tube. In other words, cicatricial stenosis occurs due to prolonged mechanical ventilation of the patient's lungs.
 Damage to the lymphadenoid and cartilaginous tissues of the respiratory tract disrupts blood circulation and leads to the development of purulent-necrotic processes in the trachea.
Damage to the lymphadenoid and cartilaginous tissues of the respiratory tract disrupts blood circulation and leads to the development of purulent-necrotic processes in the trachea.
Inflammatory reactions play a key role in narrowing the diameter of the airway.
Keloid scars formed in the ENT organs can reach a length of 3 cm.
According to the classification proposed by V.D.Parshin, according to the degree of stenotic lesion of the trachea, the following types of stenosis are distinguished:
- 1 degree - a decrease in the diameter of the trachea by no more than 30%;
- Grade 2 - a decrease in the diameter of the trachea up to 60%;
- Grade 3 - a decrease in the diameter of the trachea by more than 60%.
It should be noted that even after sparing reconstructive surgeries, the risk of re-scar formation in the cartilaginous tube remains quite high.
Therefore, corticosteroid drugs are included in the pathology treatment regimen, with the help of which it is possible to arrest purulent-necrotic processes in the tissues and, accordingly, the subsequent formation of scars.
Expiratory tracheostenosis
Expiratory tracheal stenosis (ES) is a functional decrease in the diameter of the trachea, which is associated with the immersion of the atonic film into the lumen of the cartilaginous tube. Exacerbation of symptoms is observed with attacks of a suffocating cough or vigorous breathing after exercise. In otolaryngology, there are two types of expiratory stenosis:
- primary - arises from septic inflammation of the nerve roots in the walls of the trachea; the development of the disease is often preceded by influenza, bacterial pharyngitis, laryngitis, etc.;
- secondary - develops with emphysema of the lungs, i.e. a disease that is accompanied by the expansion of the distal bronchioles and the destruction of the alveolar walls.
Dyspnea, which occurs during expiratory stenosis, is difficult to stop with the help of bronchodilators, therefore, when an attack occurs, you need to call the ambulance team.
As a rule, ES is most often diagnosed in adults over the age of 30. Typical manifestations of tracheostenosis are dry barking cough, shallow breathing, asthma attacks, fainting.Very often, a suffocating cough is accompanied by nausea and vomiting.
Diagnostics and treatment
To accurately determine the cause and degree of narrowing of the airways, it is necessary to undergo a hardware examination by an otolaryngologist. Symptoms of the pathology are nonspecific, therefore, it is necessary to differentiate tracheostenosis with bronchial asthma or the penetration of foreign objects into the throat. When conducting differential diagnostics, pulmonologists rely on the results of objective research methods, which include:
- spirography - assessment of the state of the respiratory tract, in which the volume and speed of movement of the air exhaled by the patient is measured;
- arteriography - X-ray examination of blood vessels, with the help of which the functional state of the arteries near the airways is determined;
- fibrobronchoscopy - visual examination of the tracheobronchial tree, with the help of which the degree of patency of the airways is determined;
- endoscopy - instrumental visualization of the respiratory organs, which allows you to assess the degree of stenotic lesions of the trachea;
- computed tomography - assessment of the state of the soft and cartilaginous tissues of the trachea by layer-by-layer images of ENT organs.
During the diagnosis, the specialist confirms or refutes the presence of morphological changes in the tissues of the respiratory tract. If necessary, biomaterials from the trachea are taken for biopsy in order to accurately determine the etiology of tracheostenosis.
Stenoses of organic origin require surgical treatment followed by the administration of corticosteroid drugs. Cicatricial tracheostenosis is treated with laser vaporization, balloon dilation, or bougienage. If endoscopic therapy is ineffective, scar formation is resected.
Compression tracheostenosis is much easier to treat than cicatricial. During surgery, tumors of the mediastinum, benign growths in the thyroid gland, or cysts that compress the trachea are removed. Extensive subtotal tracheostenosis can only be eliminated by tracheal transplantation.