Sometimes the heart begins to beat 4-5 times faster, and the reason for this is not a state of love or stress, but a constant form of atrial fibrillation or its paroxysmal variant. There are quite a few violations of the rhythm of the "perpetual motion machine" of our body, and this is one of them. Unfortunately, this pathology poses a serious danger to life, because in almost 30% of cases it leads to a stroke. How to prevent complications and identify the disease in time - we will discuss in this article.
What it is?
Atrial fibrillation is a rhythm disturbance in which the muscle fibers of a given part of the heart contract not just out of order, but also with a huge frequency - from 300 to 600 beats per minute. In this case, the process is inconsistent, chaotic and also leads to ventricular dysfunction. Outwardly, such a "dance" of the heart is manifested by an increase in heart rate. The latter is often difficult to feel, because it seems to flicker. It is this comparison that gave the pathology its second name - atrial fibrillation.
Next to the wording of the diagnosis on the certificate of incapacity for work, you can find the code I 48 belonging to atrial fibrillation in the ICD 10th revision.
We have to admit that, despite the tremendous advances in medicine in the treatment of this disease, it remains a key cause of stroke, heart failure and sudden death. At the same time, an increase in the number of such patients is predicted. The latter is associated with an increase in life expectancy and, accordingly, the number of elderly people suffering from arrhythmia.
What is the Difference Between Fibrillation and Flutter
I want to point out that it is a common mistake to identify these two rhythm disturbances. In fact, atrial fibrillation and atrial flutter have different origins and manifestations. The first is characterized by:
- chaotic contraction of cardiomyocytes (heart muscle cells) with different intervals between them;
- the presence of multiple foci located in the left atrium and creating extraordinary pathological discharges.
Flutter - a lighter version of arrhythmia. Although the heart rate reaches 200-400 beats per minute, the heart beats at the same time at regular intervals. This is possible due to the coordinated contraction of muscle fibers, since the impulses come from one focus of excitation. You can read more about this type of rhythm disturbance here.
Prevalence in society
Tachystolic atrial fibrillation, the most common form, occurs in 3% of adults aged 20 and over. Moreover, older people suffer from the disease to a greater extent. This trend is due to several factors:
- increase in life expectancy;
- early diagnosis of asymptomatic forms of pathology;
- the development of concomitant diseases that contribute to the appearance of atrial fibrillation.
According to the World Health Organization, in 2010, the pathology was found in 33.5 million inhabitants of the planet.
It was found that the risk of getting sick in women is slightly lower than in men. But at the same time, the former are more often prone to strokes, have a greater number of concomitant diseases and a pronounced clinic of fibrillation.
Causes of the disease and genetic aspects
I want to note that it is very important to distinguish the true cause of atrial fibrillation from factors that only contribute to the manifestation of the disease.
The pathology is based on a genetic mutation, a kind of "breakdown". Even if there are no accompanying cardiovascular risks, the chance of getting atrial fibrillation in patients with such a DNA defect is very high.
At the moment, there are about 14 variants of changes in the genotype that lead to rhythm disturbances. It is believed that the most common and significant mutation is located on chromosome 4q25.
In this situation, a complex violation of the structures and functions of the atrial myocardium occurs - its remodeling occurs.
In the future, it is planned to resort to the help of genomic analysis, which will improve the prognosis of the disease and reduce disability due to early diagnosis of pathology and timely treatment.
Diagnostics
The most informative method for diagnosing atrial fibrillation is the ECG.
But before that, the doctor will take an anamnesis. Important information will be information about:
- similar rhythm disturbances in the next of kin;
- concomitant diseases, for example, pathology of the lungs, thyroid gland, gastrointestinal tract;
- initial manifestations of menopause in women.
If the patient himself noticed an irregularity of the pulse, the doctor will ask how long these changes have been observed, and whether attempts were made to eliminate them. This is followed by a physical examination, which will immediately allow for differential diagnosis with flutter. Indeed, with atrial fibrillation, heartbeats occur at different intervals.
Listening to it will reveal the ineffectiveness of the contractions of our "engine". This means that the heart rate determined in this case will differ from the heart rate palpated on the wrist. The "floating" volume of the first tone will also attract attention. No matter how informative the physical examination is, nevertheless, in a number of cases with severe tachycardia, the doctor cannot understand the cause of the disease and give a conclusion about the irregularity of the rhythm. Then the cardiogram comes to the rescue.
ECG signs
Examination of the patient, especially in old age, using an ECG should be carried out during each visit to the doctor. This can significantly reduce the number of consequences of atrial fibrillation (ischemic stroke, acute heart failure) and improve the diagnosis of latent (asymptomatic) and paroxysmal forms. Therefore, when you are advised to undergo this procedure at an outpatient appointment or in a hospital, you cannot refuse, because many patients do not feel any interruptions in the work of the heart before the "vascular catastrophe" occurs.
New techniques are being developed that will make it possible to independently identify violations. For example, wearable skin recorders, smartphones with ECG electrodes, blood pressure monitors with built-in algorithms for detecting arrhythmias.
But all of them are still inferior in the degree of information content to the traditional cardiogram, on which the following changes are found during atrial fibrillation:
- there is no P wave;
- the R-R intervals, which are responsible for the rhythm of the ventricles, have different lengths;
- there are waves ff, considered the main symptom of the disease.
I draw your attention to the fact that to diagnose the paroxysmal form of pathology, one should resort to either a daily short-term ECG recording, or to round-the-clock Holter monitoring.
The photo below shows examples of films of people with atrial fibrillation.


Classification of atrial fibrillation
Currently, there are three classifications of atrial fibrillation used by practicing cardiologists. Pathology is divided according to:
- form (the duration of arrhythmia is meant, that is, paroxysmal, constant, persistent);
- the reason for its occurrence, or rather, by the factor contributing to its development;
- severity, taking into account the severity of the symptoms that accompany the violation of the heart rhythm.
Such a distribution is extremely important, since it allows the doctor to determine in the future the most effective way to treat the disease and prevent its secondary complications.
Forms
There are 5 forms of atrial fibrillation in national cardiology guidelines:
- first identified;
- paroxysmal;
- persistent;
- long-term persistent;
- constant.
In some patients, the disease has a progressive nature, that is, rare short-term attacks of arrhythmias gradually increase in frequency and become longer. As clinical experience shows, this situation ends in the development of permanent cardiac arrhythmias. Only 2-3% of patients can "boast" of periodic flicker for 10-20 years.
In the same section, I would like to mention the atypical form of pathology included in Frederick's syndrome. The described disease belongs to the category of tachyarrhythmias, which are manifested by an increase in heart rate and different intervals between beats. But this extremely rare type of pathology, which occurs in 0.6-1.5% of patients, is considered normosystolic and sometimes bradystolic. That is, the heart rate will be either within the normal range - 60-80 beats / min, or less than 60 beats / min, respectively.
Frederick's syndrome is a combination of fibrillation and grade III atrioventricular block. This means that the discharge from the atria simply does not reach the ventricles, the latter are excited from their own pacemaker.
Such a development of events is possible if the patient has severe organic pathologies of the heart, for example, ischemic heart disease, heart attack, myocarditis, cardiomyopathy.
First identified
Atrial fibrillation is considered for the first time, which has been diagnosed at the moment, and there is no mention of its earlier detection. This type of atrial fibrillation can be both paroxysmal and constant, asymptomatic and with a pronounced clinical picture.
You should remember that this classification form of heart rhythm disturbance is assigned regardless of the duration of the disease, which is difficult to judge in the absence of attacks of shortness of breath and palpitations, and the severity of its manifestations. And I would like to note that when you seek medical help for this pathology again, the prefix "newly revealed" will no longer appear in the wording of the diagnosis.
Paroxysmal
Paroxysmal atrial fibrillation is one that suddenly begins and disappears on its own within 1-2 days. Although there are attacks of atrial fibrillation, which persist for up to 7 days, they are also referred to this form of pathology.
With this course of the disease, patients periodically feel interruptions in the work of the heart, accompanied by shortness of breath, chest pain, weakness, dizziness, fluctuations in blood pressure. Sometimes, against the background of these paroxysms, pre-fainting conditions develop.
Persistent
Persistent atrial fibrillation is atrial fibrillation that lasts longer than a week. This also includes seizures that are eliminated only due to cardioversion or the action of medications after 7 days or more.
In practice, it is sometimes extremely difficult to differentiate between paroxysmal and persistent types, since it is not always possible for the doctor and the patient to carry out such a long ECG control. Then certain difficulties arise in choosing the most effective treatment tactics. In a number of cases, there is an alternation of these two forms of rhythm disturbance.
Long-term persistent
Long-term persistent atrial fibrillation, or persistent, "pursues" the patient for a year, and sometimes longer. The condition for such a formulation of the diagnosis is that for such a patient a cardiologist has chosen a strategy for controlling the heart rhythm. At the same time, some time after the onset of pathology, a person at rest ceases to feel the characteristic symptoms. The clinic becomes pronounced only at the time of physical exertion.
In such a situation, it is almost impossible for doctors to determine the duration of the onset of arrhythmia or the appearance of its last attack without the appropriate anamnesis or medical documentation.
Constant
A long-term persistent disease in which the doctor and the patient have decided not to take steps aimed at restoring normal sinus rhythm, subsequently acquires a different name. From that moment on, it is called a permanent form of atrial fibrillation.
This situation is possible even if attempts to "fix" the heartbeat have already been carried out, but have failed. Then interventional transcatheter radiological technologies are simply not used.
And when the patient changes his mind and agrees to measures that will lead to rhythm control, the permanent form again turns into a long-term persistent one.
Clinical classification (due to pathology)
The clinical classification is intended to differentiate atrial fibrillation by trigger factors, that is, concomitant diseases or conditions that increase the risk of arrhythmia. After all, although it was said above about the genetic cause of the pathology, this does not mean at all that it will necessarily develop. For a mutation to manifest itself, it needs to be "pushed".
The table lists situations that contribute to the development of certain types of fibrillation.
Fibrillation type | Cause |
Secondary against the background of organic lesions of the heart | It is provoked by heart disease, accompanied by left ventricular dysfunction, arterial hypertension with myocardial hypertrophy. |
Focal | It is observed in young patients with a history of atrial tachycardia or short-term episodes of atrial fibrillation. |
Polygenic | It occurs at an early age due to multiple genetic mutations. |
Postoperative | It is provoked by open cardiac surgery and usually stops on its own as the patient recovers. |
Fibrillation in patients with valve pathology | It develops with mitral stenosis, after surgical interventions to correct the valve apparatus. |
Arrhythmia in athletes | It manifests itself as paroxysms and depends on the duration and intensity of the classes. |
Monogenic | Formed in patients with a single gene mutation. |
I note that this division of atrial fibrillation by type is intended to adjust the algorithms for treating the disease.
Modified EAPC scale
This scale is used to assess the patient's quality of life, that is, it takes into account the extent to which the signs of the disease interfere with his daily work. Indeed, the severity of the clinical picture also depends on the tactics of treating atrial fibrillation.
The minimum symptoms are observed in 25-40% of patients, 15-30% - they note significant discomfort and a sharp limitation of physical activity against the background of manifestations of pathology.
The table shows the severity of atrial fibrillation.
Degree | The severity of the clinical picture |
1 | There are no symptoms of the disease. |
2a | The signs of pathology are minimal and do not interfere with the patient. |
2b | Although the patient performs daily work, shortness of breath and palpitations are already felt. |
3 | The normal functioning of the patient is disturbed as a result of severe symptoms of arrhythmia (shortness of breath, palpitations, weakness). |
4 | A patient with a given degree of severity of fibrillation is not able to self-serve. |
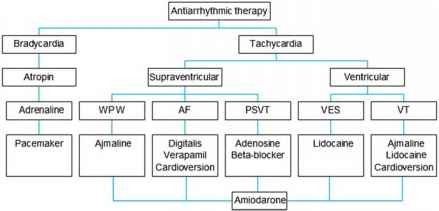
Atrial fibrillation (atrial fibrillation) treatment
Treatment of atrial fibrillation should be carried out in a comprehensive manner, that is, it is necessary to interact with primary care doctors (therapists, family doctors), to whom patients first of all turn for help, and narrower specialists (cardiologists, cardiac surgeons). Only with this approach and continuous training of the patient in the tactics of behavior in this pathology can positive results be achieved.
When choosing therapeutic measures, the following factors are taken into account:
- hemodynamic stability (blood pressure indicators), the severity of the clinical picture;
- the presence of concomitant cardiovascular and other diseases (thyrotoxicosis, sepsis, etc.), which aggravate the course of arrhythmia;
- the risk of developing a stroke and the need in this regard to prescribe drugs that thin the blood (anticoagulants);
- Heart rate and the importance of reducing this indicator;
- symptomatology of pathology and the possibility of restoration of sinus rhythm.
Only after a comprehensive assessment of the patient's condition is a decision made on the tactics of his further management.
Stroke prevention
It has long been proven that atrial fibrillation significantly increases the risk of ischemic strokes. This happens due to the formation of blood clots in the chambers of the heart, followed by their migration into the vessels of the brain.
Therefore, the treatment of a permanent form of atrial fibrillation, as well as other types of the disease, includes the use of blood-thinning drugs.
Previously, antiplatelet agents ("Aspirin-cardio", "Cardiomagnet") were prescribed to everyone practically uncontrollably in such a situation. But at present, their ineffectiveness in preventing thromboembolism has been proven. Now they resort to the use of vitamin K antagonists ("Warfarin") and new anticoagulants that are not vitamin K antagonists ("Apixaban", "Dabigatran"). Moreover, the appointment of the last group of drugs is accompanied by a lower risk of hemorrhagic strokes (intracerebral hemorrhage).
Heart rate monitoring
There are two key strategies used by practicing cardiologists to combat atrial fibrillation. One of them is aimed at controlling the heart rate, and the second is at restoring the physiological sinus rhythm. As you can imagine, the choice of tactics depends on many factors. This is the age of the patient, and the length of the illness, and the presence of serious comorbidities.
Treatment of the chronic form of atrial fibrillation in the elderly is most often based on the first of the above methods and can significantly reduce the manifestations of the disease, improve the daily activity of patients.
Removal of an attack
A rapid decrease in heart rate may be necessary against the background of newly diagnosed fibrillation and with reversible tachysystoles that occur against the background of anemia, infectious pathologies, decompensated thyrotoxicosis.
In such a situation, beta-blockers (Bisoprolol, Concor) and calcium channel blockers (Diltiazem, Verapamil) become the drugs of choice, since they have a quick action and affect the tone of the sympathetic nervous system.
In the case of a decrease in the ejection of blood from the ventricles, when arrhythmia is combined with heart failure, a combination of beta-blockers and digitalis drugs ("Digoxin", "Digitoxin") is usually used. And in patients with unstable hemodynamics, they resort to intravenous administration of "Amiodarone", which is an antiarrhythmic agent.
Means for constant admission
If there is an emergency decrease in heart rate, then, of course, there is also a long-term version of this type of therapy.
Most often, to slow the heart rate, they resort to monotherapy with beta-blockers (Metoprolol, Nebivolol, Esmolol, Carvedilol), which are well tolerated by patients of any age, regardless of the presence of sinus rhythm or fibrillation.
Calcium channel blockers, which include Verapamil and Diltiazem, although they provide heart rate control and better eliminate the symptoms of the disease, increasing exercise tolerance, are still contraindicated in chronic heart failure, accompanied by reduced ventricular ejection.
Another group of drugs prescribed for long-term use are cardiac glycosides - "Digoxin" and "Digitoxin", which have a rather toxic effect at the wrong dosage.
The antiarrhythmic "Amiodarone", to which analogs "Cordaron" belongs, is considered a reserve drug. His "services" are used extremely rarely, since his action causes a lot of side effects outside the heart.
So, to summarize: to achieve the target heart rate level, which is within 110 beats / min, the choice of funds is made individually, taking into account concomitant pathologies. And its appointment begins with a minimum dose, which is gradually increased until the desired effect is obtained.
Rhythm restoration (cardioversion)
In emergency situations, when unstable hemodynamic parameters are observed in a patient, cardiologists have the right to decide on the restoration of sinus rhythm. A similar tactic can be chosen with the usual consent of the patient, whose atrial fibrillation, while maintaining a normal heart rate, is accompanied by a vivid clinical picture (shortness of breath, palpitations, weakness, fainting).
By analogy with the above strategy, this treatment algorithm also has urgent and long-term measures. And cardioversion itself can be electrical and medication.
Emergency method
Emergency cardioversion is divided into pharmacological and electrical.
There are repeated experimental confirmations of the effectiveness of antiarrhythmic drugs in returning sinus rhythm in 50% of patients with the development of paroxysm of atrial fibrillation. At the same time, there is no need to carry out training, in contrast to the hardware method, that is, there is no need for fasting and the appointment of sedatives. The funds used in this procedure include: "Dofetilide", "Flecainide", "Propafenone", "Amiodarone", etc.
A method has been developed that allows patients to adjust their heart rate on their own at home, the so-called "pill-in-pocket" therapy. For this purpose, "Flecainide", "Propafenone" are suitable.
Electric cardioversion with direct current is chosen as the main method in patients with pronounced hemodynamic disturbances with the onset of atrial fibrillation paroxysm.
Long-term drug use
Long-term use of antiarrhythmic drugs is intended to reduce the number of symptoms associated with atrial fibrillation and improve the general condition of the patient. But, before choosing this tactic, the doctor assesses the severity of the disease, the risk of side effects and, of course, the opinion of the patient himself.
The main drugs used in this case are:
- Amiodarone;
- Dronedaron;
- Flecainide and Propafenone;
- Quinidine and Disopyramide;
- Sotalol;
- Dofetilide.
The choice of a drug is made only after a comprehensive examination of the patient and taking into account the presence of concomitant pathologies. For example, Dronedarone is contraindicated in chronic heart failure.
Catheter ablation
Catheter and radiofrequency ablation (RFA), in fact, are surgical methods in which there is an isolation of trigger zones in the pulmonary veins and "cauterization" of arrhythmogenic areas in the left atrium, that is, areas of the myocardium that can generate those very pathological discharges.
This method of restoring sinus rhythm is considered the most effective in patients with paroxysmal, persistent and long-term persistent fibrillation, accompanied by a pronounced clinical picture.Note that the procedure is resorted to only after objectively failed therapy with antiarrhythmic drugs.
Risk factors and associated diseases
So we come to the discussion of pathologies that can "push" the development of atrial fibrillation and increase the number of its relapses and complications. If these risk factors are identified in time and skillfully dealt with, many problems that arise in the treatment of heart rhythm disturbances can be avoided in the future.
Diseases that provoke atrial fibrillation include:
- chronic heart failure;
- arterial hypertension;
- pathology of the valvular apparatus of the heart;
- diabetes;
- obesity;
- respiratory diseases (COPD, sleep apnea, that is, respiratory arrest, etc.);
chronic kidney disease.
Prevention: what should the patient know?
Unfortunately, there is no specific prevention of atrial fibrillation, because drugs and technologies have not yet been developed that can fight genetic mutations. Therefore, all that remains is, as far as possible, to prevent the occurrence of diseases that provoke the development of arrhythmias.
Doctor's advice
I think there is no need to talk about lifestyle modifications that can reduce the risk of obesity, diabetes and hypertension. But many people forget that, having a family history of arrhythmia, it is necessary to treat all diseases of the lungs and bronchi in time, choose a profession wisely, avoiding work with an increased content of dust in the air (for example, the mining industry). This will reduce the risk of fibrillation associated with COPD.
Clinical case
Patient A., 25 years old, was admitted to the admission department with complaints of shortness of breath, inability to breathe deeply, palpitations, dizziness, and severe general weakness. The patient was engaged in semi-professional powerlifting, and with the next approach he lost consciousness. In the family, the grandmother and mother were diagnosed with atrial fibrillation. Objectively: the skin is pale, shortness of breath at rest, blood pressure 90/60 mm Hg, heart rate during auscultation is 400 beats / min, the first tone is also heard louder than normal, the rhythm is incorrect, the pulse on the radial artery is 250 beats / min. Provisional diagnosis: "Newly diagnosed atrial fibrillation."
To confirm the diagnosis, we used: clinical blood and urine tests, determination of the level of TSH, ECG, Echo-KG. The patient underwent pharmacological cardioversion with Dofetilide, after which the sinus rhythm with a heart rate of 60-64 beats / min was restored. During the hospital stay, daily ECG monitoring was carried out, no paroxysms of fibrillation were observed. The patient was advised to limit physical activity.