Small focal myocardial necrosis develops due to clogging of the arteries with thrombus and cholesterol plaques. It is also caused by prolonged spasm of the small coronary arteries. I often see a picture of the transferred disease on the ECG, when the person is not even aware of it. Let's take a closer look at what are the symptoms of a microinfarction in women and men and what should be done to prevent it.
Characteristics of pathology
Small focal damage to myocardial cells with subsequent necrosis occurs as a result of:
- incomplete overlap of the vessel lumen;
- the presence of collateral blood flow pathways;
- complete blockage of small arteries.
All these factors lead to unexpressed changes that rarely entail complications. But with a repeated attack or violation of the patency of several small-caliber vessels at once, the pathology can turn into a large-focal process with severe symptoms and severe consequences.
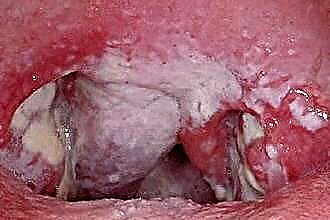
There are two types of microinfarction: intramural (located in the thickness of the myocardium and does not touch the inner and outer layers) and subendocardial (on the inner lining of the heart). In the first case, a negative T wave is recorded on the ECG in the area of violation. In the second, the ST segment shifts below the isoline, as can be seen in the photo:
First signs and symptoms
More recently, my colleagues and I considered microinfarction to be a disease that occurs mainly in men and the elderly. But as statistics and personal observations show, it is increasingly being recorded in women and people under 40.
Harbingers of an attack appear after physical or psychoemotional overstrain and in some cases resemble colds:
- weakness;
- body aches;
- temperature increase;
- a feeling of squeezing behind the breastbone.
Then the following symptoms develop:
- pain in the left side of the chest radiating to the jaw, back, under the scapula;
- blue nasolabial triangle;
- dyspnea;
- dizziness, fainting;
- frequent heartbeat.
It is important to note that the severity of the signs of a microinfarction is different. It depends on the reason for its development, the general condition of the person, his threshold sensitivity. I have observed patients with chronic diseases who get used to constant pain and weakness and simply do not notice the changes that have arisen.
Manifestations in men
Signs of a microinfarction in men are more pronounced: there is a sharp pain in the chest, there is a feeling of pressure or a foreign body. Therefore, they are more likely to seek qualified help.
When making a diagnosis, I always pay attention to the patient's appearance. In acute necrosis, there is:
- blue discoloration in the area of the lips;
- temperature increase;
- weak throbbing in the wrists;
- cold extremities;
- significant sweating.
Sometimes patients talk about only one symptom - a sharp pain in the region of the heart, which then goes away. A painless course for men is not typical.
Among women
In women, the signs of a heart attack are weak, they need to listen especially carefully to the slightest deviations in their condition. For 2-4 weeks, precursors of a microinfarction appear:
- coldness of the extremities due to impaired microcirculatory blood flow;
- the appearance of edema on the legs and arms;
- frequent urge to urinate;
- spasms in the bronchi;
- painful sensations in the stomach and a feeling of fullness;
- nausea not associated with food intake.
According to my observations, in women, the development of a microinfarction is preceded by a headache, which may be associated with increased pressure or vasospasm.
Expert advice
It is very important to recognize small focal infarction in time. It is necessary to immediately take emergency measures and call a doctor if the following signs occur:
- panic, fear of death;
- the skin is cold and clammy with sweat;
- pain in the chest on the left, gives under the scapula, in the back, jaw, half of the head;
- the pulse is felt poorly or is not detected;
- the nasolabial triangle turns blue.
You also need to know that sometimes (especially in diabetics and the elderly), small focal infarction proceeds without symptoms or manifests itself in the form of asthma attacks, abdominal pain, rhythm disturbances. But any form can turn into a large-focal or transmural infarction, therefore it requires urgent qualified assistance.
Disease prevention
To prevent the disease, the following rules should be followed:
- Undergo an annual examination and take a cardiogram. This is a prerequisite for people over 45 years old.
- Control body weight. This will help reduce the stress on the heart and prevent the development of type II diabetes.
- Exercise regularly. This improves the general condition of the body and optimizes metabolic processes. A trained heart can more easily tolerate pressure surges and the release of catecholamines during a stressful situation.
- Refrain from smoking and alcohol abuse.
- Control blood pressure and sugar levels, treat hypertension or diabetes in time.
- Revise the menu towards a healthy diet, reduce the consumption of salt and animal fats.
Secondary prevention consists in the constant use of Aspirin, statins and beta-blockers. During the recovery period, you should gradually increase physical activity, perform exercise therapy exercises and walk in the fresh air.
Treatment
The provision of care for a microinfarction should be carried out only in the cardiology department of the hospital. The task of my colleagues is to stop the pain syndrome, localize the focus of necrosis and take measures so that the heart can work as usual.
The following groups of drugs are used for treatment:
- anticoagulants;
- neuroleptanalgesia or narcotic analgesics;
- polarizing mixture, droppers with glucose and salt solution;
- beta blockers;
- antiarrhythmic drugs;
- prolonged nitrates.
The patient is advised to follow bed rest, a diet with the exception of salt and fatty foods. Physical, mental and social rehabilitation is desirable after discharge. If the patient's professional activity is associated with constant overload, he is sent to the commission for transfer to an easier job.
Consequences of a microinfarction
The prognosis depends on the speed of assistance and the implementation of the specialist's recommendations to the patient - both during the acute period and during rehabilitation. But a certain area of tissue is not fully restored and can no longer perform its usual function. Even after adequate treatment, there is a risk of complications:
- thrombosis is repeated with the appearance of multiple small foci and extensive necrosis begins;
- acute, and then chronic heart failure develops;
- calcinate forms at the site of the lesion;
- the left ventricle is enlarged;
- rhythm and conduction disturbances occur;
- unstable angina appears.
According to statistics, in 30% of cases after the first microinfarction, a repeated episode occurs and leads to a large-focal lesion of the heart muscle. Complications are especially common in patients with diabetes mellitus and severe atherosclerosis.
Case from practice
A 54-year-old woman came to the clinic with complaints of weakness and nausea. The problem was associated with malnutrition. During the survey, it turned out that she had been suffering from exertional angina for 10 years, attacks occur several times a month and were stopped by "Nitroglycerin".
The ECG shows signs of acute ischemia along the lower wall of the left ventricle, without the formation of a Q wave. Diagnosis: Small focal infarction.
The woman underwent a full course of treatment in the hospital, her condition improved, she was discharged under the supervision of a local cardiologist. Recommended: dieting, taking Aspirin Cardio, Metoprolol, Atrovastatin.