Grade 3 throat cancer is characterized by the most pronounced clinical signs. In this regard, the diagnosis of the disease often occurs during this period.
Grade 3 throat cancer is characterized by the most pronounced clinical signs. In this regard, the diagnosis of the disease often occurs during this period.
Particular attention to this disease is due to the performed function of the larynx to move air into the lower parts of the respiratory tract.
With the development of a volumetric process in the larynx, blocking the path of inhaled air, the patient may die from suffocation. All this creates a need for an earlier diagnosis of laryngeal cancer.
Diagnosis of the disease
The course of laryngeal cancer and its prognosis depend on factors such as the localization of the process, the stage of the disease. Diagnostic measures are aimed at clarifying these factors.
According to its composition, the larynx is divided into
- upper section;
- middle, vocal cords;
- lower, lining department.
Diagnosis of cancer of the vocal cords and the upper larynx is quite simple and relies on the results of laryngoscopy performed by a specialist in an ENT office. However, in the case of localization of the tumor in the lower, subglottic region, the results of the indirect laryngoscopy may be insufficiently reliable.
The larynx in the lower regions is less amenable to visual inspection. In addition, patients with such a localization of the process seek advice from an otolaryngologist at later stages, since the symptomatology in this case is atypical. Differential diagnosis with laryngitis, laryngotracheitis or diseases of the larynx caused by specific pathogens is possible only on the basis of additional examinations.
In the event that the results of indirect laryngoscopy do not give a reliable result, direct laryngoscopy is performed to clarify the diagnosis. It consists in the introduction of a laryngoscope on a flexible hose directly into the lower, lining of the larynx. Further research using a magnifying technique allows you to get a more specific idea of the changes occurring in the mucous membrane.
 At the initial stages, the pathologically altered area looks like an insignificant tubercle, towering over a site of healthy tissue. When a tumor grows into the epithelial layer, injected vessels can alert a specialist. The third stage in the development of laryngeal cancer is histologically characterized by the growth of the tuberosity of the epithelial layer, which captures all parts of the larynx. A lesion in the third stage of laryngeal cancer may appear as an erosive surface prone to bleeding. To further clarify the nature of the process, it is necessary to carry out a microscopic examination of the affected tissue area, for which a biopsy is performed. The reliability of the study is estimated at 100%.
At the initial stages, the pathologically altered area looks like an insignificant tubercle, towering over a site of healthy tissue. When a tumor grows into the epithelial layer, injected vessels can alert a specialist. The third stage in the development of laryngeal cancer is histologically characterized by the growth of the tuberosity of the epithelial layer, which captures all parts of the larynx. A lesion in the third stage of laryngeal cancer may appear as an erosive surface prone to bleeding. To further clarify the nature of the process, it is necessary to carry out a microscopic examination of the affected tissue area, for which a biopsy is performed. The reliability of the study is estimated at 100%.
Hardware technology is used among other diagnostic methods. X-ray examination of the chest organs allows you to detect metastases in the lungs, assess their number and size. Magnetic resonance imaging and computed tomography can be used, which consists in a layer-by-layer examination of organs in order to detect metastases in them.
Ultrasound of the neck allows you to more accurately determine the size and density of regional lymph nodes. This is especially important when it comes to deeply located lymph nodes that are inaccessible to palpation.
Clarification of the prevalence of the tumor process is an important diagnostic factor that allows you to choose the correct treatment method.
Clinical signs
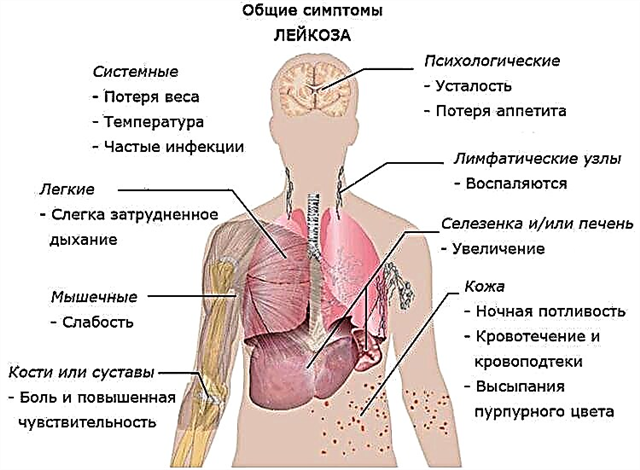
The third stage of laryngeal cancer is characterized by the progression of symptoms. At this stage, all parts of the larynx can be involved in the process, therefore the clinical picture is characterized by a variety, indicating the spread of the process. The patient complains about
- persistent sore throat, aggravated by swallowing;
- sensation of a foreign body in the throat;
- malaise and weakness;
- losing weight;
- shortness of breath;
- change in the timbre of the voice, the development of aphonia;
- dry paroxysmal cough, difficulty breathing;
- asthma attacks;
- hemoptysis;

- fetid odor from the mouth.

There is a swelling of the neck due to an increase in regional lymph nodes. They are presented in the form of dense bags welded to the surrounding tissues. A diagnostic biopsy allows detecting atypical cells in the lymph nodes, indicating the development of regional metastases. As for other organs, the studies carried out exclude the presence of metastases in them.
Treatment principles
The task of specialists in choosing treatment tactics in the third stage of laryngeal cancer is complicated by the fact that, due to the prevalence of the tumor, the removal of the affected organ can lead to a violation not only of sound production, but also of vital functions and respiration. At the same time, independent use of other methods of treatment, chemotherapy and radiation, will be ineffective.
Treatment for stage III laryngeal cancer is complex and includes surgical removal, chemotherapy, and radiation therapy.
The most radical method of surgical treatment of a patient in this case is the removal of the entire larynx, cervical tissue and adjacent lymph nodes.
The larynx is brought up and cut off. After the introduction of the nasoesophageal probe, the edges of the wound are sutured together.
After the surgery, the patient can breathe on his own. However, remote vocal cords prevent the pronunciation of sounds. To restore this function, prosthetics can be performed in the future.
For the relief of the tumor process in the larynx, good results are noted with the use of X-ray radiation. Therefore, to obtain the maximum effect, radiation therapy is often performed before or after surgical removal. However, it should be borne in mind that the use of radiation therapy after surgery complicates the postoperative course.
The latest modern technique used to treat cancer patients is photodynamic therapy (PDT).
It consists in the local introduction of a photosensitizer into the affected area. In this case, only cancer cells interact with a chemical dye, leaving healthy tissue unused. Then radiation of a certain frequency is directed to the affected area, which interacts exclusively with the cells marked with the dye.
As a result of exposure to radiation, oxidation and destruction of cancer cells occurs. Given this selectivity of action, the technique is characterized as a promising direction in the treatment of oncopathology.
A comprehensive approach to the treatment of stage III laryngeal cancer helps to prolong life by 5 years for half of the total number of patients.